
Medicine
HGVS nomenclature
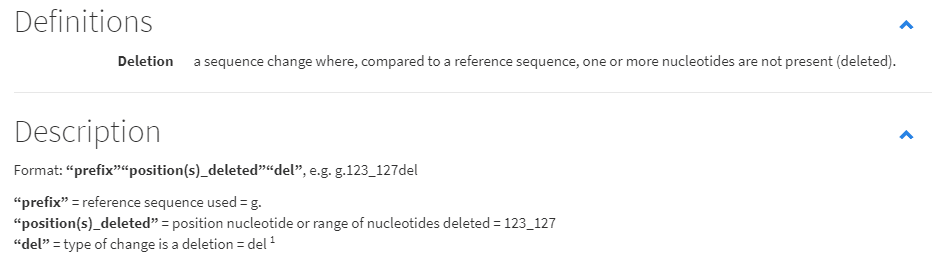
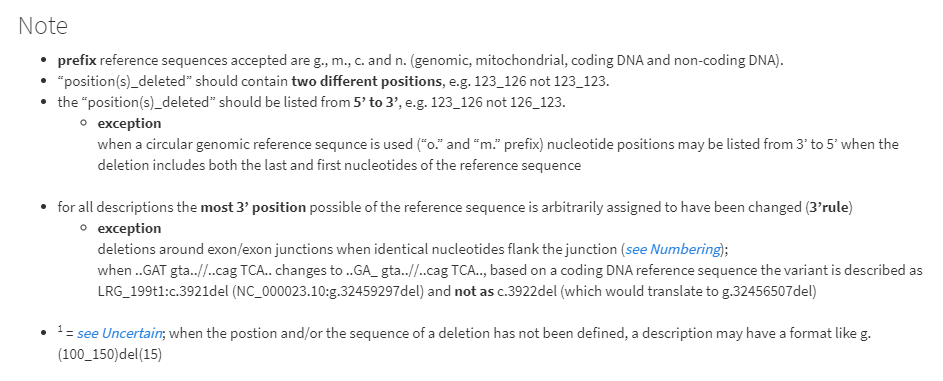
HGVS stands for Human Genome Variation Society. Its nomenclature for genetic mutations is accepeted by most of the reseach institutes and sciencific societies. The complete information can be checked on the page below:
https://varnomen.hgvs.org/
Hope it be useful for future doctors and biology scientists!
Gene deletion, homozygous or heterozygous?
Chromosome mutations often arise in cancer cells, and we shall see several cases in this chapter and the next. As an example, Figure 17-8 shows some deletions consistently found in solid tumors. Not all the cells in a tumor show the deletion indicated, and often a mixture of different chromosome mutations can be found in one tumor. The contribution of such changes to the cancer phenotype is not understood.
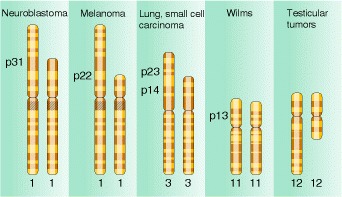
Deletions found consistently in several different types of solid tumors in humans. Band numbers indicate recurrent breakpoints. (After Jorge Yunis.)
Homozyous deletions are usually lethal, while heterozygous deletions could be also dangerous.
Deletions can happened on single gene (intragenic) or several genes (multigenic). Some deleted mutations are still viable.
In our case, we should determine the precise location of gene deletion (now proved to be a exon 9 homozygous deletion)
P.S. As to our case, it can be categorized as an exon deletion case. About exon deletion, the most famous related disease is DMD(Duchenne Muscular Dystrophy).[2] The mutations (including exon deletion) happen on the gene called dystrophin gene.[3]
Reference:
[1]Griffiths AJF, Miller JH, Suzuki DT, et al. An Introduction to Genetic Analysis. 7th edition. New York: W. H. Freeman; 2000. Deletions. Available from: https://www.ncbi.nlm.nih.gov/books/NBK21904/
[2]https://www.parentprojectmd.org/about-duchenne/what-is-duchenne/types-of-mutations/
[3]https://en.wikipedia.org/wiki/Dystrophin
Epidemics Homework
2019 novel coronavirus disease (COVID-19) has become a vital hygienic issue for China’s health system. And as a critical part of the disease control, diagnosis is of importance to local hospital and epidemic prevention departments of other provinces. The protocols of diagnosis of COVID-19 have changed during the different phases in this nation-wide plague. The reasons and the probability of such changes may be an interesting stuff to review. Hence I will review the diagnosis standards and guidelines in this passage.
Based on what we have learnt in the MOOC, the diagnosis of epidemic is consisted of evidences from clinical data, epidemic data and laboratory examinations. As to COVID-19, “the protocol of diagnosis and treatment of COVID-19 infected-pneumonia” has six editions. The first edition mainly focused on the epidemic data, of which was “exposure in Huanan seafood market”. The clinical traits were restricted to respiratory system, although several research late or early had shown multiple-organs-related lesions.[1] The laboratory and radiology examinations generally supported an initial diagnosis of virus-infected pneumonia.
It’s clear that the first edition on 16th January failed its responsibility. This protocol didn’t help the health systems nationwide to stop the spreading of this virus. For people who may be infected by a former one with exposure to Huanan market, the epidemic standard was neglected.
Skip to the 5th edition, the diagnosis standards have changed a lot. The standards were divided into two parts, one for residents in Hubei province and the other for the rest parts of China except Hubei. On respective of Hubei, so-called “clinical standards” have been added, due to the former edition mainly focused on the nucleic-acid detection and RT-PCR examinations, which widened the diagnosis limitation of suspected cases. The “clinical standard” made the symptoms of heating and respiratory system as the enrolling standard, together with complete blood counts and regardless of “epidemic data”. The confirmed cases’ standards stayed still.
Such changes are deleted in the 6th edition. The difference between people within or without Hubei is removed, which means the epidemic data again becomes the necessary part of diagnosis for resident in Hubei. The importance of Chest CT have been iterated. [2]
Between the alternation of 6th to 5th, the confirmed the suspected cases among the whole country, even in Hubei, had declined hugely. Was it a miracle of China’s health system and government’s eligibility, or a diagnostic trick to prettify the arrival of new rule? It requires time and more research to witness.
Reference
[1] https://www.medrxiv.org/content/10.1101/2020.02.08.20021212v1
[2] Ai, T., Yang, Z., Hou, H., Zhan, C., Chen, C., Lv, W., . . . Xia, L. (2020). Correlation of Chest CT and RT-PCR Testing in Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology, 200642. doi:10.1148/radiol.2020200642